

Roger Greenhalgh (top left), Stéphan Haulon (top right), Ludovic Canaud (bottom left), and Gustavo Oderich (bottom right)
This week, the CX 2020 LIVE agenda turned to the technically challenging topic of aortic arch interventions. Through presentations, discussion, and polling, the session—chaired by Roger Greenhalgh (London, UK) and moderated by Stéphan Haulon (Paris, France)—aimed to tackle some vital questions, including how to reduce the risk of stroke in thoracic aortic endovascular procedures, what the best options are for the left subclavian branch, and how best to approach aortic arch aneurysms. The session covered atherosclerosis, dissection, transection and ulcers, and their role in guiding treatment was clearly emphasised, with audience polling revealing that 85% would alter reconstruction in the arch according to the underlying pathology. The session also dealt with the wider debate of open versus endovascular surgery and considered the benefits of a multidisciplinary team. In a boost for the endovascular approach in this difficulty anatomy, 63% of audience members disagreed with the statement “Open is best”.
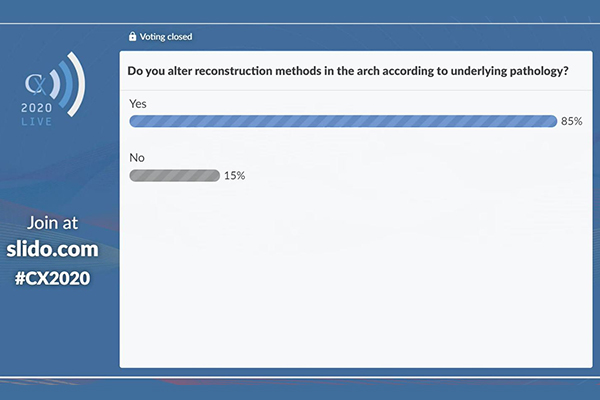
CX 2020 LIVE polling results
Gustavo Oderich (Rochester, USA) outlined preliminary experience with a range of device options that would enable the left subclavian artery [LSA] to stay patent. He began with the statistic that “30–60% of thoracic endovascular aortic repair [TEVAR] patients require Zone 2 incorporation with coverage of the LSA”. Considering the implications, he detailed: “We know LSA coverage without revascularisation is associated with more arm ischaemia, posterior circulation events, and spinal cord injury”.
He noted that patient-specific fenestrated stent grafts have been available for over two decades, and added that reports from the Cleveland Clinic and the Hamburg group demonstrate that mortality and stroke can be an issue, particularly if there is misalignment of the stent graft requiring arch manipulations.
Considering options for left subclavian branch incorporation, Oderich began with the Terumo Aortic Scallop stent graft, outlining a Dutch registry of 30 patients showing “excellent outcomes”, with only one Type Ia endoleak, one mortality, and one stroke.
Moving on to the Gore Thoracic Branch Endoprosthesis (TBE), he noted that this is currently under investigation in the USA. “This device has a single retrograde portal and one-side branch stent,” he said, adding that “this is a self-expandable stent, specially designed for the subclavian artery, with flared diameters”.
“It is recommended for these cases to obtain brachiofemoral through-and-through access for better support of the side branch,” he told the CX 2020 LIVE audience, going on to detail his clinical experience: “My preference is to use a small incision to expose the distal brachial artery, obtain retrograde access, and snare the wire in the distal thoracic aorta. The device has been loaded via the aortic wire and the through-and-through brachiofemoral wire”.
Oderich detailed that the feasibility trial results with the Gore TBE were reported in the Annals of Thoracic Surgery, with “excellent outcomes for Zone 2, no mortality, one minor stroke, one late asymptomatic subclavian artery branch occlusion, no Type Ia endoleak, and no late neurological events”.
Going on to discuss the Medtronic Valiant Mona LSA stent graft, Oderich outlined that this was investigated in an early feasibility study of nine patients. “Although technical success was obtained in all patients, there were three minor non-disabling strokes,” he detailed.
The Cook LSA single branch device, which Oderich noted was designed by Stéphan Haulon (Le Plessis-Robinson, France) and colleagues, has a triple-wide scallop that incorporates the left carotid artery and a preloaded catheter. “Following deployment of this stent graft, a sheath is advanced via the preloaded catheter, the subclavian artery is catheterised, and the repair is extended with a bridging stent,” he described.
He concluded: “Zone 2 extension is needed in up to 60% of TEVAR patients, and the preliminary experience with LSA branch devices indicates low morbidity and stroke rates, with high patency rates”.
 Global audience seeks expert opinion on LSA branch devices
Global audience seeks expert opinion on LSA branch devices
In the discussion following his presentation, Oderich first addressed a question from Haulon on treatment with an off-the-shelf device. He responded: “We can have an off-the-shelf device for the subclavian artery, because the location of the left subclavian artery in relation to the left carotid artery is quite predictable”.
He continued: “I do think that a lot of these patients currently being treated with coverage will actually have the option of revascularisation. That would include acute cases, like dissection or even transection. In the pivotal trial from Gore, the enrolment has been quite fast for the chronic dissection group. It is quite impressive. They were tentatively trying to enrol 10 patients and they have already included 93. So, I think that there will be a large subset of patients that will benefit from the left subclavian branch”.
An audience member watching from Moldova then asked Oderich, “In what subgroup of patients would either a bypass or transposition be used rather than a branch endograft?” to which Oderich responded that the “obvious” cases would be when the subclavian artery is not suitable for a branch.
Oderich noted that, given the investigational nature of some grafts, surgeons are still “shying away” from treating patients with certain indications, for example a very dominant vertebral artery. That being said, “with increased experience, as we showed, the patency rate is excellent”. He was positive looking forward: “I do think there will be a benefit of a branch over a bypass”.
One limitation of branches may be for the low origin of the left vertebral artery, Oderich revealed in a response to a question from Brighton, UK. In these cases, “we have to consider another device, like a scallop subclavian artery incorporation,” he suggested.
Finally, a question from Singapore asked when you would choose an LSA branch device over a fenestrated one for the LSA. “The issues with fenestration are several-fold,” Oderich responded. “First of all, from the standpoint of industry, it becomes [a] totally patient-specific device for the most part. The nice think about the branches is the ability to deploy the aortic stent graft and commit to that position. You do not have to keep twisting and you can just focus on the branch.
“I would say people are probably going to move away from fenestration towards a branch,” he concluded.

Roger Greenhalgh (top left), Stéphan Haulon (top right), Roberto Chiesa (bottom left), Philippe Charbonneau (bottom centre), and Luca Bertoglio (bottom right)
Collaboration needed to respond to aortic arch aneurysms
Roberto Chiesa (Milan, Italy) provided a comprehensive overview of total endovascular, hybrid, open and frozen elephant trunk repair techniques, looking at which is the best strategy to use in different scenarios, and the European Society for Vascular Surgery (ESVS) recommendations for each. He stressed: “The clever surgeon chooses the best option for the patient.”
Chiesa’s key message on aortic arch aneurysms was the need for multidisciplinary decision-making. He revealed that, at his centre, meetings take place every day between vascular and cardiac surgeons to decide on the choice of technique. Chiesa’s message also illustrated the potential that exists for using patient characteristics to choose between endovascular and open reconstruction. This view was reflected in the polling result on whether to alter reconstruction in the arch according to underlying pathology, with which 85% of respondents agreed. “It [the approach chosen] depends on the extent of the disease and the situation of the patient. In a fit patient, also in a young patient … open surgery can represent a good option. Endovascular repair offers possibilities that open surgery cannot offer,” he said.
“Acceptable results in fit patients” can also be achieved using the Frozen Elephant Trunk technique, said Chiesa, describing a hybrid strategy—a combination of both open and endovascular technique—as “a good option in high to moderate-risk patients”, and total endovascular branch repair as providing improving results in anatomically suitable patients. He closed his presentation with the prediction: “I think that will represent the future.”
Chiesa’s colleague, Luca Bertoglio (Milan, Italy), also presented an edited case of a carotid subclavian bypass. He explained that LSA revascularisation is recommended in aortic procedures to reduce the incidence of spinal cord ischaemia and stroke. Bertoglio noted this was the procedure that “we prefer to perform in our centre”.
He outlined how the carotid subclavian bypass is performed, and dealt with common difficulties encountered, including the impact of anatomy on the choice of implant.
A lively discussion followed his presentation, at the end of which Greenhalgh declared himself to have “been extremely entertained”.
Kevin Mani (Uppsala, Sweden) echoed Chiesa’s comments on the need for consultation with cardiothoracic colleagues when he discussed the feasibility of endovascular arch repair for type A dissection. He explained that more than two-thirds of post type A dissection repair patients are technically eligible for endovascular arch repair. He said: “It is not an easy procedure for the surgeon or the patient, so everybody is happy if it can be done endovascularly at the second stage.”
He concluded: “More than two-thirds of post type A dissection repair patients are technically eligible for endovascular arch repair. Future advancements that may increase this number include a greater awareness among cardiovascular surgeons of a sufficient ascending graft length.
“Considering the high rate of eligible patients, it can be expected that the use of endovascular arch repair for type A dissection patients will increase over time and increasingly replace redo sternotomy as the treatment of choice,” Mani speculated.
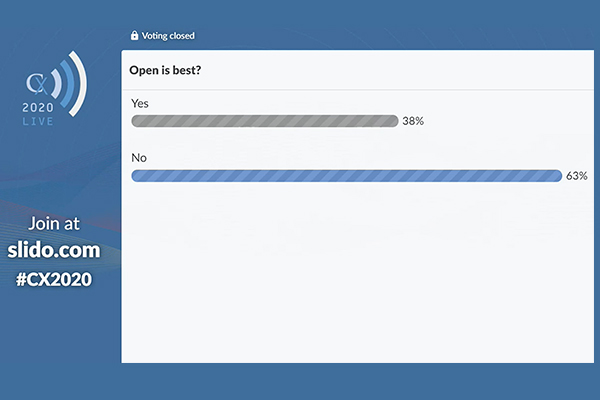
CX 2020 LIVE polling results
Silent cerebral lesions study: Clinical stroke incidence small but infarction rate “substantial” on magnetic resonance
Philippe Charbonneau (Paris, France) presented findings from a multicentre study which looked to quantify silent cerebral lesions, evaluate their clinical impact and to identify predictive factors following endovascular arch repair. He noted that TEVAR is the primary repair technique for aneurysms of the descending thoracic aorta but added that “neurological complications from this technique remain a significant concern” with the stroke rate at around 5%.
The study found that a total of 245 silent cerebral infarcts were detected in 45 patients, which represented almost 50% of the cohort. Lesions were multiple in 78% with a “predilection for both hemispheres” (58%) as opposed to isolated hemispheres (33% left and 9% right). When comparing baselines characteristics between patients with and without silent cerebral lesions, “no difference was found on univariate analysis”. An operative analysis of patients with and without new lesions showed that urgent procedure, deployment in Ishimaru zone 0–1, placement of a branch or fenestrated endograft, a proximal stent diameter of more than 40mm and the use of a haemodynamic strategy during the deployment were all “significantly associated with the presence of ischaemic lesions”.
Haulon said the results are “really interesting” and noted that there is “room for improvement” in aortic arch repair procedures. After Charbonneau fielded questions from physicians across the globe, Greenhalgh remarked that “The STEP study was set up for this very reason” and concluded that the “key is to see whether we can modify technique to reduce that [the infarction rate].”
Double fenestrated stent graft associated with low risks of mortality and persistent stroke
During the session, Ludovic Canaud (Paris, France) described the double branch technique as the “gold standard” for endovascular repair of the arch, while acknowledging that it does carry a high risk of mortality, failure, and stroke. An alternative approach is the chimney procedure, Canaud said, noting that while this is associated with high technical success, it has also been known to carry a risk of endoleak that is higher than 20%. Canaud also outlined the current status of in situ fenestration, detailing its high technical success rate on the one hand, but also issues with long-term follow-up on the other, including fabric tears and poor-quality fenestration.



