
The CX ilegx Collaboration Day course has been designed to update attendees on the latest treatment strategies developed to avoid the increasing number of unnecessary lower limb amputations—flagship principles of the ilegx initiative. Delegates will learn about the King’s College Hospital open access vascular diabetic foot care pathway—an effective approach which incorporates early diabetic foot referral and interdisciplinary work—which is showing promising results saving limbs.
Delegates will also hear about revascularisation strategies of the ischaemic foot with the latest data in the field; and will have the opportunity to discuss in more detail, in two roundtables led by experts, the controversy of “Leaving something in” or “Leaving nothing behind” in the superficial femoral artery. This subject will be exposed in the CX Main Programme – Peripheral Arterial Controversies (two days before ilegx).
In the commentary below, Michael Edmonds (King’s College Hospital, London, UK), who is one of the founders of ilegx and co-director of the CX ilegx Collaboration Day course, explains the King’s College Hospital pathway. He also writes about the value of endovascular techniques for diabetic foot care and critical limb ischaemia treatment.
This is followed by an interview with Cliff Shearman (University of Southampton, Southampton, UK), co-director of the ilegx Collaboration Day. He talks about what he believes the take-home message from this year’s CX ilegx Collaboration Day will be.
Commentary by Michael Edmonds, ilegx course director
Early referral, fast track care and multidisciplinary work: Key approach to save limbs
The ilegx Collaboration Day will include an account of a modern successful approach to the diabetic ischaemic foot in the King’s College Hospital (London, UK) open access vascular diabetic foot care pathway, which has resulted in greater than 90% limb salvage rate.
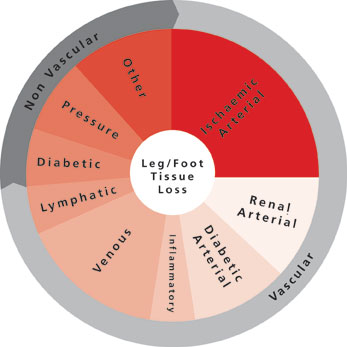
This approach is based on a new understanding of the natural history that has led to a novel classification of the ischaemic diabetic foot, emphasising the importance of the diabetic neuroischaemic foot as well as the critically ischaemic foot. This pathway is operated by an interdisciplinary team comprising surgeon, physician, podiatrist, nurse and orthotist and provides integrated care focused on a diabetic foot clinic. The diabetic foot can deteriorate with alarming speed and for this reason the clinic provides open rapid access to accelerate urgent assessment and to proceed quickly to state-of-the-art interventions in the revascularisation of not only the critically ischaemic foot but also the neuroischaemic foot. This includes prompt decision making within the interdisciplinary team as to proceed to endovascular or open vascular surgery (or both in a hybrid technique), involving revascularisation of both legs and increasingly, pedal arteries. The diabetic neuroischaemic foot is particularly characterised by ulceration and complicating infection and within this interdisciplinary diabetic foot service, modern techniques in wound care and aggressive treatment of infection with surgical debridement and parenteral antibiotics are also important.
The value of endovascular techniques for diabetic foot care and critical limb ischaemia treatment
There is a crucial role for endovascular techniques to revascularise the foot, whether it is to restore blood flow in order to help diabetic ulcers to heal, or longer-term as a treatment for critical limb ischaemia.
It is agreed that the critically ischaemic foot should be urgently revascularised so as to save the limb either by endovascular procedures or open vascular surgery. However, controversy exists when there is a diabetic patient with a neuroischaemic foot ulcer that is not healing in a moderately ischaemic limb. These patients are often not getting the benefit of endovascular procedures in a timely fashion.
Although the neuroischaemic foot would not have got into trouble unless it had been subjected to minor trauma—which is often unsensed because of nerve damage—it is important to understand that, having got into trouble, the ulcer cannot be healed because the blood supply to the foot cannot be increased. Thus there is a crucial role for below-the-knee endovascular procedures to improve the blood supply, even if it is a temporary increase, to get such ulcers healed. Once such ulcers are healed it will not matter if subsequently there is restenosis.
Interview with Cliff Shearman, ilegx course director
In this year’s CX iLegx Collaboration Day, what do you think the take home message will be?
Shearman: Avoiding amputation is relatively easy; it is about early treatment and not ignoring the problem. The biggest barrier to success is poor organisation and lack of awareness of the seriousness of the problem. Solving the problem improves outcomes, improves quality of care and saves a lot of money.
This year’s ilegx roundtables will discuss revascularisation strategies in the superficial femoral artery; do you believe you should “Leave nothing behind” or “Leave something in”?
Shearman: Better understanding of the biology of diabetic vascular disease will lead to better therapies. While it is appealing to consider therapies, which do not leave anything behind, we have to understand what the main effect (short- and medium-term) of an intervention is on the plaque to design the optimum therapy.
About ilegx
The ilegx initiative, launched in 2008, was created in response to the increasing number of lower limb amputations which are mostly due to type II diabetes.
ilegx is a collaboration of like-minded health professionals, patients and care workers who share the view that too many legs are amputated and many of these are completely unnecessary.
The ilegx mission is to attract attention and draw awareness to the need for an improvement in health care in order to lower unnecessary major amputation of legs.
The CX ilegx Collaboration Day will take place at the Charing Cross Symposium on Thursday 30 April – Grey Learning Centre, Olympia Grand, London, UK
Click here to see the CX Main Programme Sessions
Click here to see the CX Parallel Sessions
Click here to register



